Artiss [Fibrin Sealant (Human)]: The Use of Fibrin Sealants for Skin Grafts in Burn Surgery
O.R. Insights Blog
Artiss [Fibrin Sealant (Human)]: The Use of Fibrin Sealants for Skin Grafts in Burn Surgery
The treatment of burn injuries with skin grafts can be traced back to 750-800 BC with the earliest documented use by the surgeon Sushruta.1 Autologous skin translocation, also known as “skin grafting,” has played an important role in burn wound management and has a rich history of its own. 1 In fact, some of the oldest known medical texts describe these ancient methods of skin translocation in detail. 1 Tangential excision and autologous skin graft coverage is a foundational principle in burn surgery.2 In terms of covering the excised wounds, autologous split-thickness skin grafts have evolved as being optimal for full-thickness dermal defect coverage.2 Over the last decades, the use of fibrin sealant has gained popularity as a graft fixation method.2
This article will provide an overview of Artiss [Fibrin Sealant (Human)], a slow-polymerizing fibrin sealant that consists of two plasma-derived components: a sealer protein solution and a thrombin solution, by exploring its mechanism of action, key clinical findings, and providing guidance on use.3 Whether you're already familiar with this fibrin sealant as a skin graft adhesion method, or want to learn more, Dr. Steven Kahn† of the Medical University of South Carolina, will delve into the role it has played in burn surgery, exploring its impact on enhancing graft fixation and patient outcomes.
Artiss [Fibrin Sealant (Human)] is a fibrin sealant indicated to adhere autologous skin grafts to surgically prepared wound beds resulting from burns in adult and pediatric populations greater than or equal to 1 year of age. Artiss [Fibrin Sealant (Human)] is indicated to adhere tissue flaps during facial rhytidectomy surgery (face-lift).
Artiss [Fibrin Sealant (Human)] is not indicated as an adjunct to hemostasis.
Click here for the Indications and Important Risk Information and accompanying Prescribing Information.
Introduction
Over the years, mortality and morbidity in burn surgery have improved significantly.2 Nevertheless, besides burn resuscitation and fluid replacement, the concept of tangential excision and immediate coverage remains rule number one in the approach of a burn patient.2 In terms of covering the excised wounds, autologous split-thickness skin grafts have evolved as being optimal for full-thickness dermal defect coverage.2
Sutures and staples have been used as the standard method of fixation.2 Staple removal can cause pain and anxiety in the patient and frequently requires intravenous analgesia and/or sedation, and in some instances conscious sedation or general anesthesia.4 The use of fibrin sealant has gained popularity as a graft fixation method because of the well-known adhesive properties.2 Because fibrin sealants are eventually broken down via the same mechanisms used in blood clot dissolution, they don't require additional healthcare visits for removal, making them an attractive alternative to staples or sutures.4
The only fibrin sealant currently indicated for skin graft fixation in burn surgery is Artiss [Fibrin Sealant (Human)] which has a slow-setting formulation to allow sufficient time for graft positioning.3,4 In 2018, we presented an abstract at the American Burn Association Annual Meeting describing an “enhanced recovery” burn surgery paradigm that utilized Artiss [Fibrin Sealant (Human)] fixation for 32 skin grafts with no (or minimal staples/sutures) without graft loss.5 We routinely use it in our practice now, and perform increasingly large and complex grafts without staples or sutures, even on functional, mobile areas such as hands.
Selected Risk Information: Artiss [Fibrin Sealant (Human)] is contraindicated in individuals with a known hypersensitivity to aprotinin and/or hypersensitivity to any of the active substances or excipients, including proteins such as fibrinogen, thrombin and human albumin.
Key Properties of ARTISS [Fibrin Sealant (Human)]
It provides full surface adherence of a skin graft to the wound bed.3,4
It decreases incidence of seroma/hematoma without requiring follow-up for staple/suture removal.3*
*Compared to standard of care
What is ARTISS [Fibrin Sealant (Human)]?
Artiss [Fibrin Sealant (Human)] received approval from the United States (US) Food and Drug Administration (FDA) in 2008.3 It consists of two plasma-derived components, a sealer protein solution and a thrombin solution.3 The sealer protein solution contains human fibrinogen 67-106 mg/mL, fibrinolysis inhibitor (synthetic) 2250-3750 KIU/mL and total protein 96-125 mg/mL.3 Human thrombin 2.5-6.5 IU/mL and calcium chloride 36-44 μmol/mL are components of the thrombin solution.3 Both compounds are provided frozen in two preloaded syringes presented in a single spraying device ready for topical application after thawing.3
What is the Indication?
Artiss [Fibrin Sealant (Human)] is indicated is indicated to adhere autologous skin grafts to surgically prepared wound beds resulting from burns in adult and pediatric populations greater than or equal to 1 year of age.3 It is also indicated to adhere tissue flaps during facial rhytidectomy surgery (face-lift).3 Artiss [Fibrin Sealant (Human)] is not indicated as an adjunct to hemostasis.3

How Does It Work?
Upon application, the fibrinogen is transformed into a fibrin matrix that adheres to the wound surface and to the skin graft to be affixed (Video 1).3,4 The adhesive properties of Artiss [Fibrin Sealant (Human)] provide full surface adherence of the graft to the wound bed, minimizing the dead space that exists when grafts are attached using point fixation techniques such as staples.4 It decreases the incidence of seroma and hematoma, and full surface adherence minimizes areas of dead space between the wound bed and applied tissues.3
Potential Advantages of a Slow-Setting Fibrin Sealant
Fibrin sealants that do not have a low thrombin concentration begin to polymerize almost immediately.6
Artiss [Fibrin Sealant (Human)] has an extended polymerization time providing up to 60 seconds to manipulate and position the graft.3
Video 1. ARTISS [Fibrin Sealant (Human)] Mechanism of Action
Clinical Evidence for ARTISS [Fibrin Sealant (Human)]
Clinical Evidence: Pivotal Study
The efficacy of Artiss [Fibrin Sealant (Human)] versus staples for skin graft adherence was demonstrated in a Phase 3, multicenter, prospective, randomized, evaluator-blinded clinical trial in 138 adult and pediatric burn patients.4 The study was designed to evaluate the rate of complete (100%) wound closure achieved 28 days after wound excision and sheet skin grafting when Artiss [Fibrin Sealant (Human)] or staples were used.4
Results demonstrated the proportion of test sides with complete wound closure was similar between the two treatments.4 Complete wound closure was defined as total coverage (including areas healing be secondary intention).4 Artiss [Fibrin Sealant (Human)] was at least as efficacious as staples for complete wound closure at day 28 (at a one-sides 97.5% confidence interval) as tested by the prospectively defined primary efficacy analysis.4
Patients had a significant preference for Artiss [Fibrin Sealant (Human)] over staples as it provides reduced pain and anxiety.4 Investigator satisfaction with graft fixation was also monitored at day 14, day 28, and month 12.4 The overall level of satisfaction with graft fixation was significantly higher for Artiss [Fibrin Sealant (Human)] over staples at all time points (P < 0.0001).4 In addition, investigators were significantly more satisfied with the overall quality of healing with Artiss [Fibrin Sealant (Human)] as compared to staples (P < 0.0001; Figure 1).4
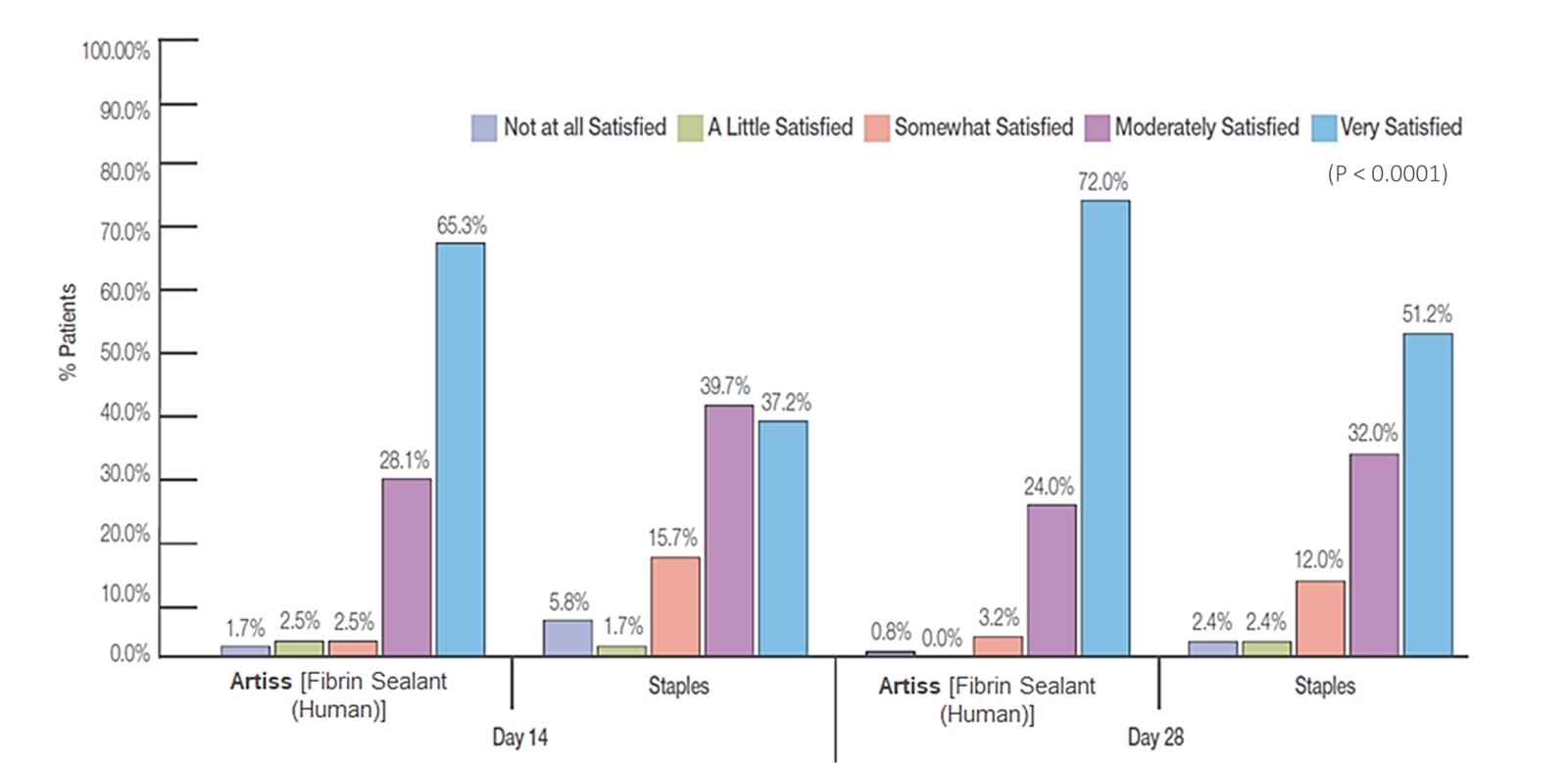
Disclaimer: Graph adapted from Foster et al.4
Clinical Evidence: Retrospective Study of ARTISS [Fibrin Sealant (Human)] vs. Staples
A retrospective single-center, single-surgeon frequency-matched cohort study was completed by Kerckhoven and colleagues on 83 patients with thermal injury burns covering 1%-25% of total body surface area, requiring early excision and immediate coverage with split-thickness skin grafts.2 Grafts were fixated with either Artiss [Fibrin Sealant (Human)] only or staples only. Primary outcome parameters included the requirement of pain medication for postoperative pain and the need for narcosis for postoperative procedures.2
Graft-fixation with Artiss [Fibrin Sealant (Human)] resulted in a decrease in administration of analgesics (P=0.005) and anesthetics (P=0.007) postoperatively (Figure 2). Artiss [Fibrin Sealant (Human)] proved to be a safe and effective alternative to staples for graft fixation.2 It demonstrated benefits in short-term burn outcomes by reducing the need for analgesics and anesthetics postoperatively.2
Figure 2. Requirements for Analgesics and Anesthetics for Graft Fixation2
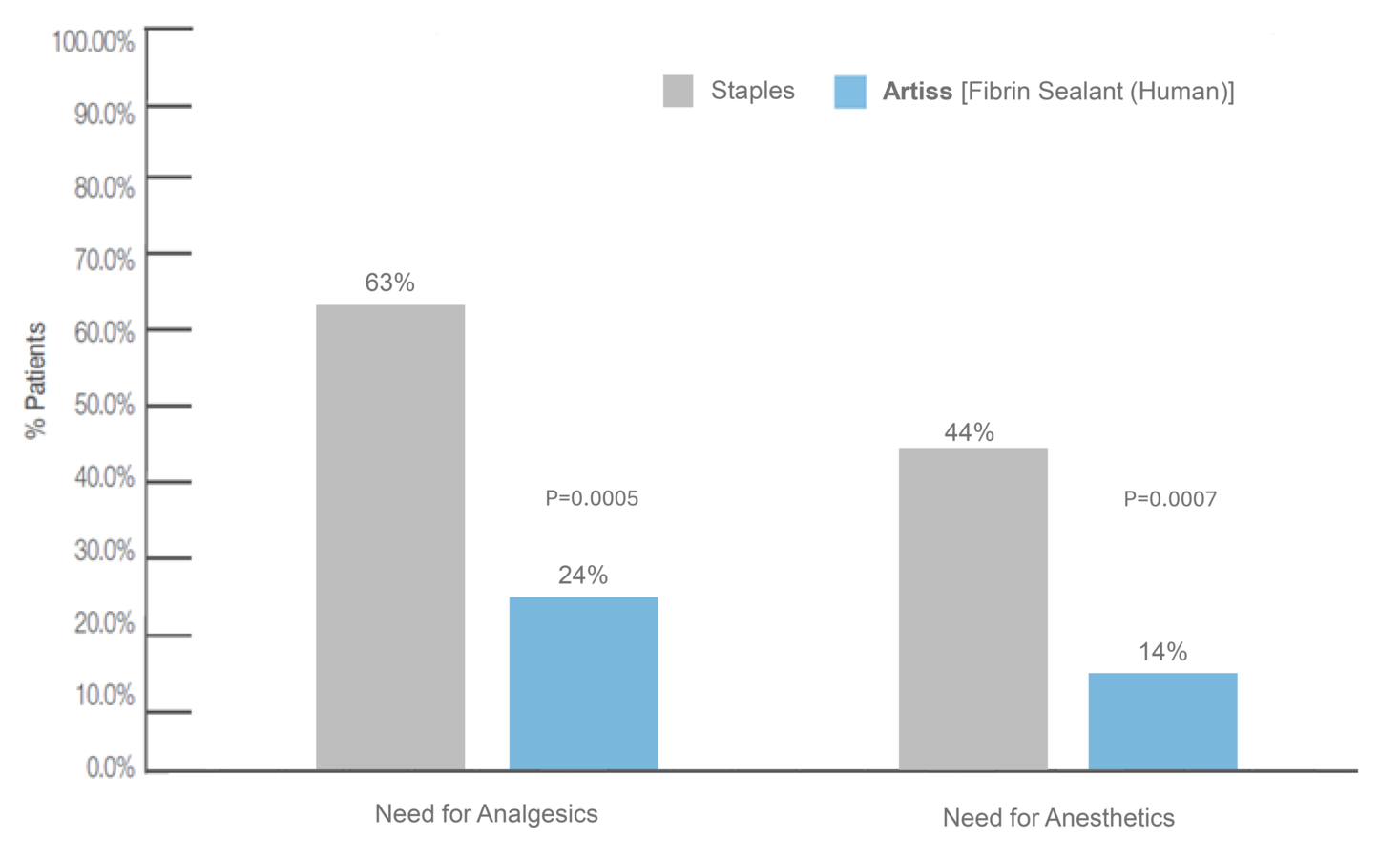
Graph adapted from Van Kerchhoven et al.2
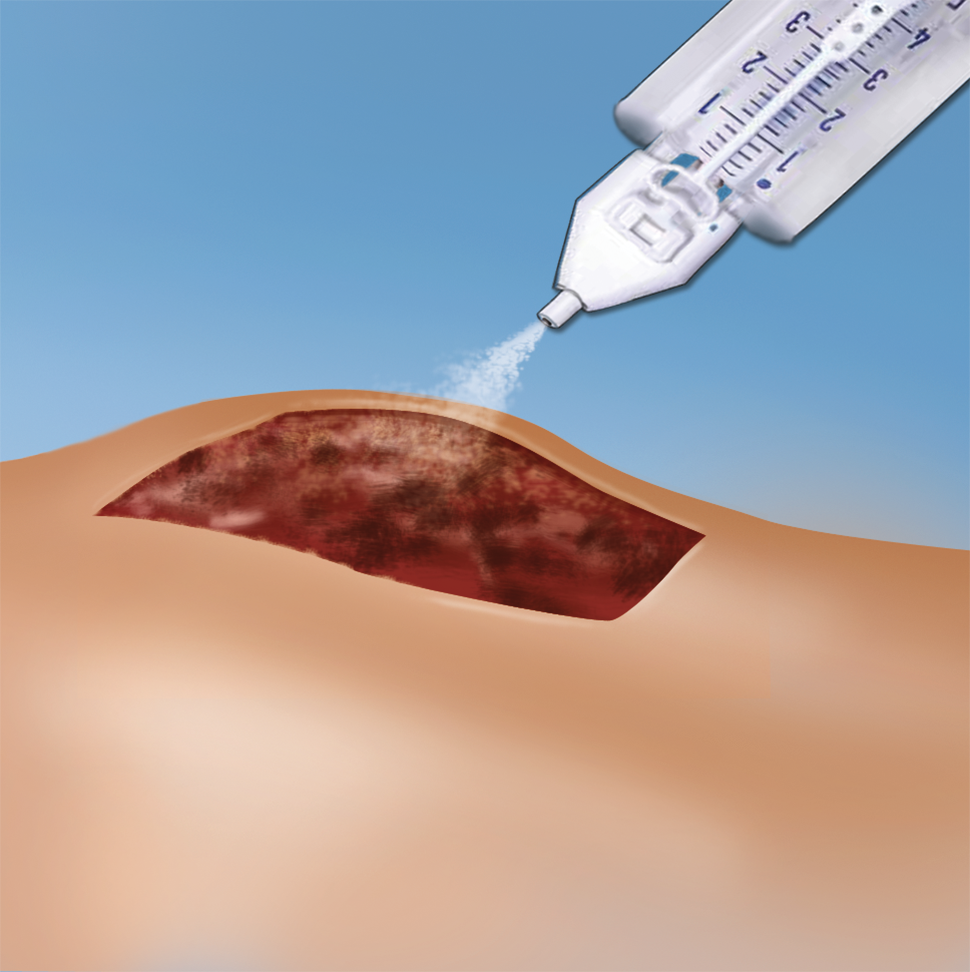
Application of ARTISS [Fibrin Sealant (Human)] for Skin Grafts

Figure 3. Split thickness skin graft being applied with Artiss [Fibrin Sealant (Human)]3

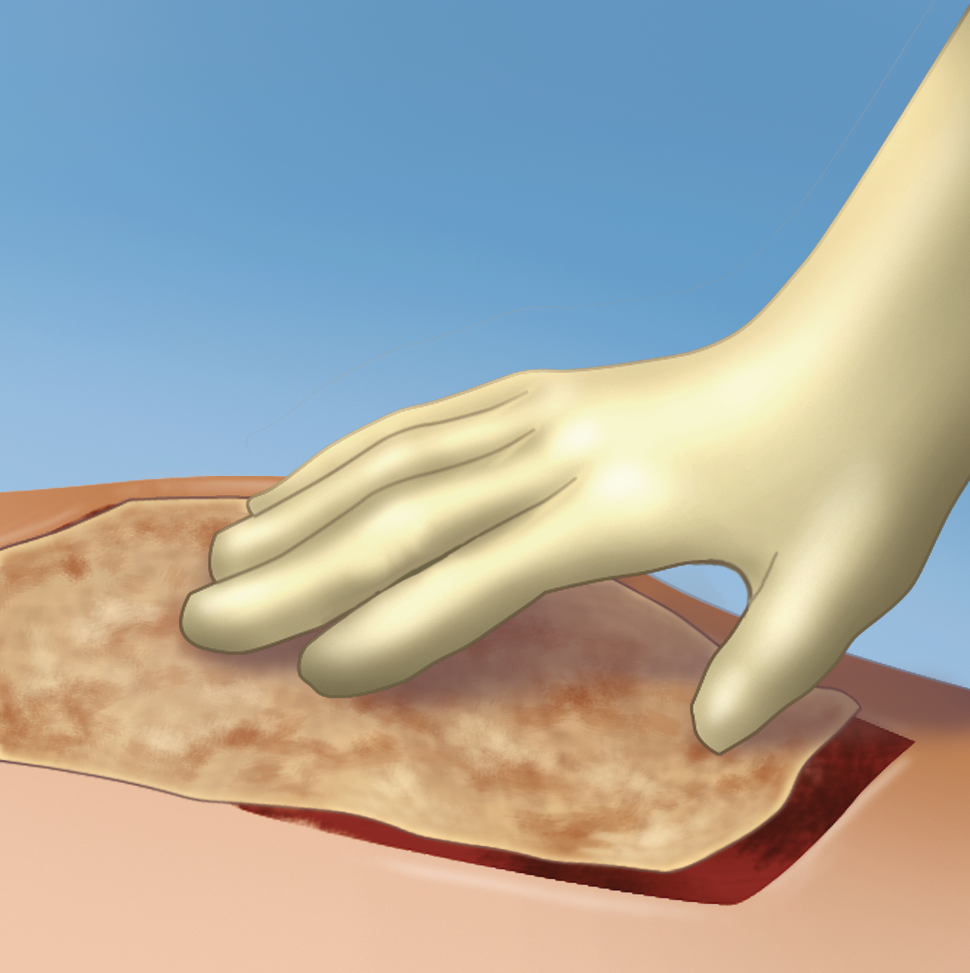
Figure 4. The graft is laid out flush with the wound bed.
Selected Risk Information for ARTISS [Fibrin Sealant [Human]}: Do not spray where the minimum recommended distance from the applicator trip to the target site cannot be assured.
Summary
In summary, Artiss [Fibrin Sealant (Human)] decreases incidence of seroma/hematoma.3,4 It sets in approximately 60 seconds, allowing time to manipulate and position graft prior to polymerization, and allows for full surface adherence of the graft to the wound bed eliminating dead space.3 The pivotal clinical study demonstrated that Artiss [Fibrin Sealant (Human)] is at least as efficacious as staples for complete wound closure by day 28 (at a one-sided 97.5% confidence interval).4
In addition, investigators were significantly more satisfied with the overall quality of healing with Artiss [Fibrin Sealant (Human)] as compared to staples (P < 0.0001).4 Graft-fixation with Artiss [Fibrin Sealant (Human)] also resulted in a decreased need for administration of analgesics and anesthetics postoperatively.2
†Dr. Kahn was compensated for his time developing this blog.
ARTISS [Fibrin Sealant (Human)] Indication
ARTISS [Fibrin Sealant (Human)] Indications
Artiss [Fibrin Sealant (Human)] is a fibrin sealant indicated in adult and pediatric patients to:
- Adhere autologous skin grafts to surgically prepared wound beds resulting from burns
- Adhere tissue flaps during facial rhytidectomy surgery
<u>Limitations of Use</u>
Artiss [Fibrin Sealant (Human)] is not indicated as an adjunct to hemostasis
Important Risk Information
- For Topical Use Only. Do not inject directly into the circulatory system or into highly vascularized tissue. Intravascular application can result in life-threatening thromboembolic events and can increase the likelihood and severity of acute hypersensitivity reaction in susceptible patients.
- Do not use in individuals with a known hypersensitivity to aprotinin and/or hypersensitivity to any of the active substances or excipients of Artiss [Fibrin Sealant (Human)].
- Do not spray where the minimum recommended distance from the applicator tip to the target site cannot be assured.
- Hypersensitivity reactions, including anaphylaxis, can occur. Should symptoms occur, discontinue and administer appropriate treatment. Such reactions may especially be seen if product is applied repeatedly over time or in the same setting, or if systemic aprotinin has been administered previously; however, these reactions may also occur in patients receiving Artiss [Fibrin Sealant (Hutman)] for the first time.
- Aprotinin is known to be associated with anaphylactic reactions. Even in the case of strict local application of aprotinin, there is a risk of anaphylactic reactions to aprotinin, particularly in the case of previous exposure.
- Discontinue administration in the event of hypersensitivity reactions. Remove the already applied, polymerized product from the surgical field.
- Life threatening/fatal air or gas embolism has occurred with the use of spray devices employing pressure regulator to administer fibrin sealants. This can occur if a spray device is used at higher than recommended pressures and in closer than recommended proximity to the tissue surface. To reduce the risk of potential life-threatening gas embolism, spray using only the appropriate pressurized gas at the recommended pressure (21.8-29.0 psi) and distance (10-15 cm). Use the EasySpray device, or an equivalent spray device cleared by FDA, connected to a medical grade CO2, Compressed Air or Nitrogen. The risk appears to be higher when fibrin sealants are sprayed with air, as compared to CO2. Spray only onto visible application sites, not in enclosed body cavities.
- Artiss [Fibrin Sealant (Human)] may denature when exposed to solutions containing alcohol, iodine or heavy metals. If these substances have been used to clean the wound area, the area should be thoroughly rinsed and dried before application of Artiss [Fibrin Sealant (Human)].
- Artiss [Fibrin Sealant (Human)] is made from human plasma, it may carry the risk of transmitting infectious agents, e.g., viruses, the variant Creutzfeldt-Jakob disease (vCJD) and theoretically, the classic Creutzfeldt-Jakob disease agent.
- Most common adverse reactions reported in ≥ 1% of clinical trial subjects with the use of Artiss [Fibrin Sealant (Human)] were: Skin graft failure, hematoma and pruritus in burn studies, and hematoma/seroma in rhytidectomy studies.
Please see accompanying full Prescribing Information for Artiss [Fibrin Sealant (Human)] at: https://baxterpi.com/pi-pdf/Artiss_PI.pdf
Baxter and Artiss are registered trademarks of Baxter International Inc. or its subsidiaries.